Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
Our hospital treats a variety of knee disorders (illnesses) and injuries (traumas). We perform surgical treatment when conservative treatments do not improve symptoms or when surgical intervention is expected to worsen the condition. We offer a wide range of procedures, from minimally invasive procedures using an endoscope (an arthroscope displayed on a high-definition 4K monitor) to direct vision (not arthroscopic) procedures to correct bow legs and preserve the joint, and total knee replacement. The reason we offer such a wide range of procedures is that even with the same disease, each patient's condition is different, and their lifestyles, such as age, activity level, and occupation, differ. Therefore, in order to propose and implement treatments tailored to each individual, we believe it is necessary to be familiar with and utilize a variety of surgical techniques.
| Endoscopic (arthroscopic) surgery |
|
|---|---|
| direct vision surgery (Joint-preserving surgery,artificial joints) |
|
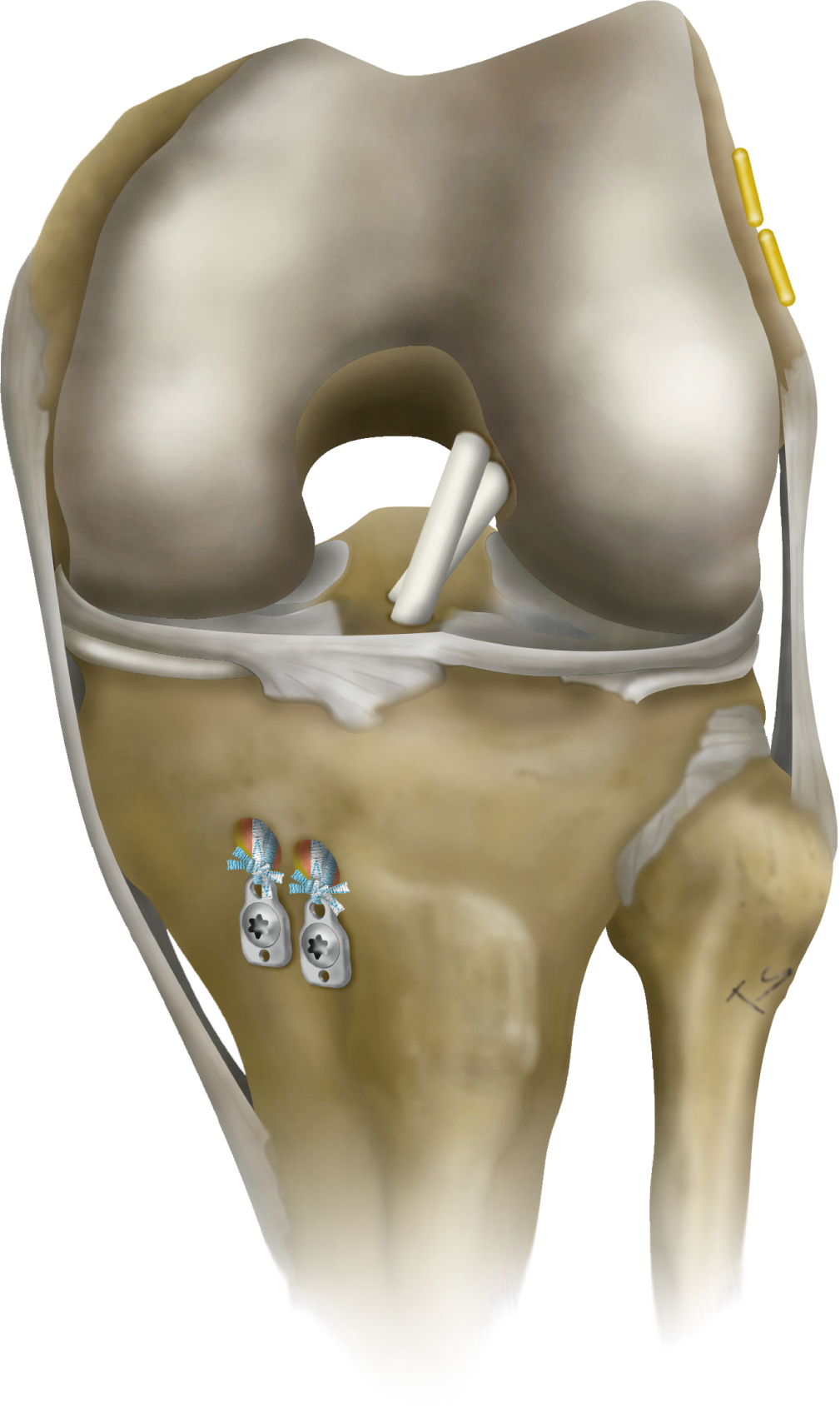
Cruciate ligaments are ligaments located in the center of the knee and include the anterior cruciate ligament and posterior cruciate ligament. When damaged, they cause instability in both the front and back of the knee, but they also cause instability in terms of twisting. In particular, anterior cruciate ligament injuries are prone to causing symptoms of instability such as knee collapse, and if left untreated, they can lead to osteoarthritis, so surgery to reconstruct the ligament is often necessary. At our hospital, we perform double-bundle reconstruction using hamstring tendons or reconstruction using a bone-attached patellar tendon, depending on the patient. We perform surgery to reconstruct the ligament as close to its original form as possible.
The meniscus is a tissue in the knee that acts like a cushion, and when damaged, it can cause symptoms such as pain, a catching sensation, and in some cases, locking (a condition in which the knee feels caught and becomes painful, making it impossible to bend or straighten the knee). While conservative treatment can sometimes improve symptoms, surgery is often the only way to alleviate the symptoms. Because the meniscus does not regenerate once it is gone, we do not perform resections lightly, and instead strive to suture the meniscus whenever possible, preserving it. However, in cases where the meniscus is in poor condition or in elderly patients, where suturing is difficult or there is a high risk of re-tear, we may perform a partial resection, leaving as much of the meniscus intact as possible.
In addition, meniscus damage often accompanies bowed legs, and if there is a high possibility of recurrence with meniscus treatment alone, osteotomy may be performed in combination.
Cartilage is a smooth tissue that covers the joint surface, but as damage progresses, the bone becomes exposed on the joint surface, causing pain. For advanced cartilage damage, we mainly perform autologous osteochondral transplantation, in which healthy bone cartilage (a part that does not bear weight) is harvested from the same knee and transplanted into the affected area. If the area of damage is small, it is possible to perform the procedure endoscopically, but if the area of damage is large, it may be necessary to open the joint.
It is mainly performed for osteoarthritis of the knee and idiopathic osteonecrosis of the femoral condyle.
Knee osteoarthritis is a disease caused by the wear and tear of cartilage, resulting in bone deformation. It is common in older people, but can also occur in relatively younger people due to meniscus or ligament damage.
The exact cause of idiopathic osteonecrosis of the femoral condyle is unknown, but it often occurs in the medial femoral condyle. It is thought to be caused by blood flow disorders and microfractures. It develops with severe pain, and the bone may collapse rapidly.
If symptoms such as pain do not improve despite conservative treatments such as exercise therapy, drug therapy, and bracing, surgery may be necessary.
Many Japanese people have varus knee deformities (bow legs), and if the bone deformity is limited to the inside of the knee, it may be possible to treat it by performing surgery to correct the shape of the tibia (shin bone) (high tibial osteotomy).The advantage of this surgery is that it preserves the patient's original knee, making it possible to reconstruct a knee that is close to its natural state.
At our hospital, we make smaller incisions in the skin than before and use plates that are tailored to the bone structure of Japanese people to firmly fix the bones, which shortens the rest period after surgery and also allows the wound to heal quickly, allowing patients to return to their daily lives and work more quickly than before.
For idiopathic osteonecrosis of the femoral condyle, autologous osteochondral transplantation may be used in combination to directly treat the necrotic area.

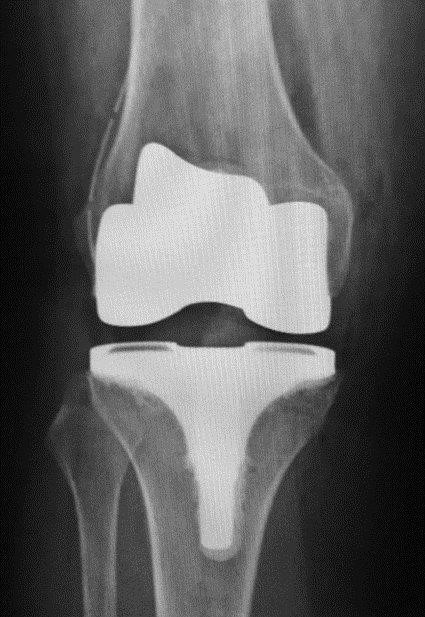
Total knee replacement surgery is performed when the deformity has spread to the entire joint, when the patient is not very active, or when the patient is elderly. The requirements for an artificial joint are that it allows stable movement without pain and that it is durable over the long term. Therefore, when performing total knee replacement surgery, we not only thoroughly evaluate the knee itself using CT scans before surgery, but also evaluate the condition of the entire lower limb, and aim to place the artificial joint in the correct position. We also strive to perform the surgery carefully, sparing as much of the tissues that support the joint, such as ligaments, as possible.