Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
Our hospital is certified as a "Primary Stroke Center" by the Japan Stroke Society, and is open 24 hours a day, 365 days a year to accept patients with strokes including cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage. Our stroke physicians can promptly begin tPA and thrombectomy. Our neurosurgery and neurology departments work together to operate the stroke center, with five stroke specialists and four neuroendovascular specialists working full-time. Our stroke care unit (SCU) has nine beds, making it one of the largest in Osaka Prefecture. Our team of physicians, nurses, physical therapists, occupational therapists, speech therapists, and pharmacists provides medical care to patients, helping them return to society as quickly as possible.
Neuroendovascular treatment is a catheter-based non-incision treatment that has made rapid progress in recent years. It includes thrombectomy for cerebral infarction, coil embolization for cerebral aneurysms, and stent placement for carotid artery stenosis. Our hospital actively performs these treatments, and when the benefits and risks to patients are comparable to those of craniotomy, we recommend neuroendovascular treatment as the first option.
Cerebral aneurysms are swellings formed at the branching points of blood vessels that supply the brain, and the cause of most cases is unknown. When an aneurysm has not ruptured (an unruptured aneurysm), it rarely causes any symptoms. However, large unruptured aneurysms can cause symptoms (such as double vision or decreased vision) due to compression of the surrounding nerve tissue.
Unruptured cerebral aneurysms are often found by chance during imaging tests such as brain checkups, and the number of such cases has been increasing in recent years. The decision to treat an aneurysm or wait and see is made after thorough consultation and consideration of the risk of rupture based on factors such as age, aneurysm size, and location.
If an unruptured cerebral aneurysm were to rupture, it could cause a subarachnoid hemorrhage. Subarachnoid hemorrhage can often result in death or severe after-effects, so our hospital is equipped with a 24-hour emergency treatment system.
There are two main types of treatment for aneurysms: craniotomy and endovascular therapy. Craniotomy involves drilling a hole directly into the skull to expose the aneurysm and then clipping it. Endovascular therapy involves guiding a thin tube called a catheter from a blood vessel in the groin or arm to the head, where a coil is inserted into the aneurysm from within the blood vessel to cut off blood flow (for details, please see the Q&A on treatment below).
Cerebral infarction is a disease in which a blood vessel in the brain suddenly becomes blocked, causing the brain tissue beyond the blockage to die and lose function. Typical symptoms include "sudden loss of strength in one of the limbs," "slurred speech (difficulty speaking)," and "sudden darkness and difficulty seeing in one eye." Symptoms may improve if treatment is administered before the brain completely dies, so it is important to start treatment as soon as possible.
If symptoms appear within 4.5 hours, we will administer t-PA therapy (a drug that dissolves blood clots). Furthermore, if symptoms appear within 24 hours, we may perform thrombectomy, which uses a catheter to remove the blood clot. These treatments require a large number of medical staff, and our hospital is able to provide t-PA therapy and thrombectomy 24 hours a day.
Causes of cerebral blood vessel blockage include arteriosclerosis, which is an aging phenomenon of blood vessels, and arrhythmias such as atrial fibrillation. To prevent arteriosclerosis, it is important to properly treat lifestyle-related diseases such as high blood pressure, diabetes, obesity, and dyslipidemia, and to quit smoking. For arrhythmias such as atrial fibrillation, treatment will be provided in consultation with our cardiology department.
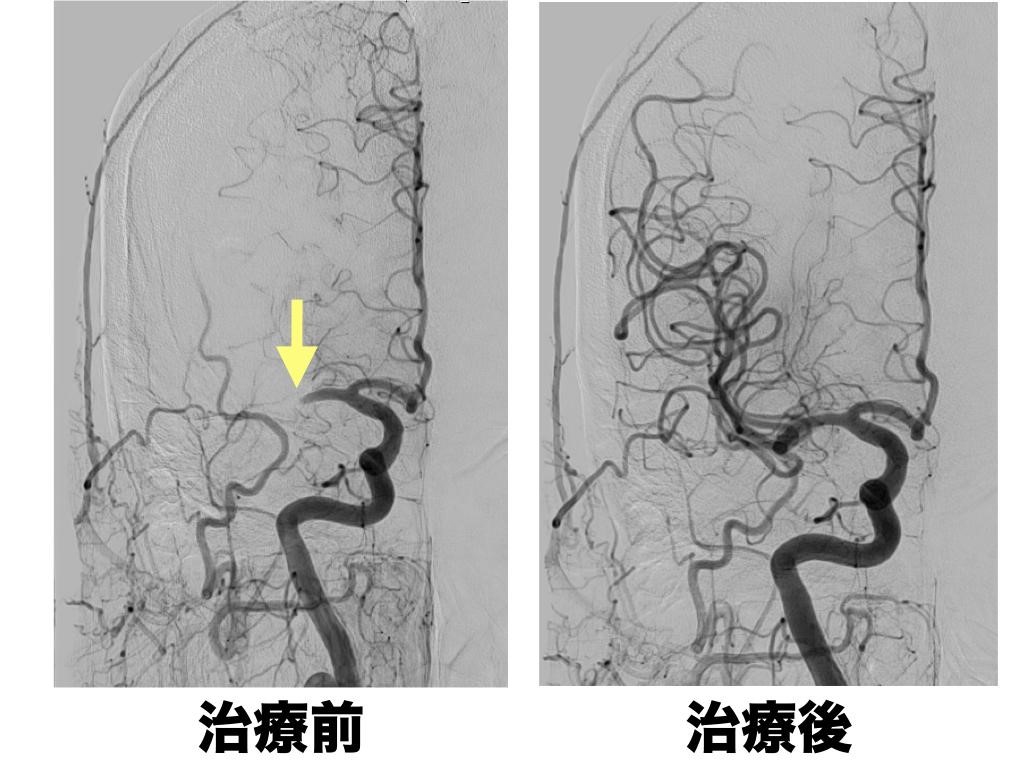
The right middle cerebral artery was occluded (arrow), but was recanalized after t-PA treatment and endovascular therapy. Symptoms improved rapidly and eventually almost completely disappeared.


Thrombus retrieved with a stent-type thrombectomy device
Formerly known as "cerebral hemocytosis," this condition occurs when small blood vessels in the brain rupture, causing bleeding within the brain. This condition disrupts brain tissue in the area of bleeding, and blood clots compress the surrounding brain tissue, impairing neurological function. High blood pressure is often the cause, but it can also be caused by cerebral arteriovenous malformations or dural arteriovenous fistulas. Depending on the size and location of the bleeding and the symptoms, emergency surgery may be considered for life-saving purposes. Surgery is performed using craniotomy or neuroendoscopy.
It is a congenital cerebral vascular malformation, a disease in which an abnormal vascular network forms between arteries and veins. It does not often cause symptoms, but it can lead to intracerebral hemorrhage or seizures. It may also be discovered by chance during a brain checkup. If intracerebral hemorrhage occurs, treatment is required. Depending on the condition, treatment may involve a combination of craniotomy, endovascular therapy, and radiation therapy.
In case of type 1, imaging tests are performed every six months to one year to check for any changes in the size or shape of the cerebral aneurysm. It is important to control blood pressure and quit smoking.
For type ii, there are two options: craniotomy, which involves clipping the aneurysm, or using a catheter and embolic material (coils) to seal the aneurysm from the inside. While craniotomy is considered highly reliable, it is also considered to be physically and mentally stressful for the patient. Endovascular treatment involves guiding a very thin catheter to the lesion and filling it with coils to cut off blood flow and prevent bleeding. As mentioned above, our hospital recommends endovascular treatment when the patient's benefits and treatment risks are comparable between craniotomy and endovascular treatment. Depending on the location and shape, endovascular treatment may be more risky, and craniotomy may be recommended. To accurately determine the shape and location of the cerebral aneurysm, detailed examinations such as contrast-enhanced CT and cerebral angiography are performed, and a comprehensive judgment is made to select the most appropriate method.
Please consult with your doctor in detail regarding the appropriate treatment. We also have a system for getting a second opinion, so please feel free to use it.

An example of endovascular treatment for the brain
The ruptured cerebral aneurysm was treated with endovascular therapy (coil embolization), and the aneurysm was filled with coils. After the procedure, blood flow to the aneurysm disappeared.

An example of craniotomy
The aneurysm wall was thinned in some places. The aneurysm was exposed, the surrounding blood vessels were left intact, and the blood flow into the aneurysm was blocked with a clip.