Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
| attending physician | Dr. Yoshihisa Suzuki |
|---|---|
| Outpatient | Facial paralysis reconstruction outpatient clinic (2nd and 4th Thursdays) |
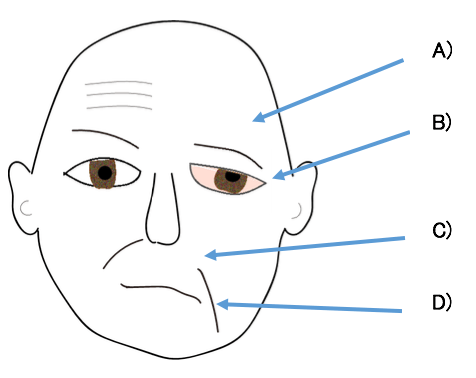
The facial nerve is the nerve that controls the movement of the muscles that create facial expressions (facial muscles).
The facial nerve is divided into four branches: the temporal branch, the zygomatic branch, the buccal branch, and the marginal mandibular branch. When the nerve is paralyzed, various symptoms appear. Sometimes all the nerve branches are paralyzed, and sometimes only certain parts are paralyzed.
Regarding laughter reconstruction, if there is a possibility of natural recovery, reconstruction will be considered about one year after the paralysis. If there is a low possibility of natural recovery, aggressive surgery will be performed early, as the shorter the time since paralysis, the less likely the facial muscles will atrophy.
If keratoconjunctivitis is caused by lagophthalmos, there is a risk of blindness, so it is important to perform surgery as soon as possible. Our department is one of the few facilities nationwide that also performs corneal sensation reconstruction surgery in cases where lagophthalmos has caused conjunctival congestion or corneal ulcers. This surgery can weaken the movement of the eyelids closing in response to pathological synkinesis (involuntary eyelid closure).
Paralysis of the temporal branch causes the eyebrow to droop lower than the healthy side. Excess skin on the side of the eyebrow is removed.
However, the eyebrows do not move like they do on the healthy side, so there is a difference between the left and right sides when making expressions that involve raising the eyebrows or closing the eyes.
Fascia lata is harvested and transplanted under the skin of the cheek to lift the nasolabial folds (laugh lines) and lips.
The upper eyelid also droops due to ptosis of the eyebrows, so excess skin is removed.
The lower eyelid also turns outward due to drooping of the cheek, so it is lifted by transplanting auricular cartilage or fascia lata.
When the eyes cannot be closed (lagophthalmos) due to paralysis of the orbicularis oculi muscle that closes the eyelids, it may be necessary to adjust the upper eyelid as well as lifting the lower eyelid.
Temporalis muscle transfer: In cases of lagophthalmos, this is a method in which part of the temporalis muscle is moved to the upper and lower eyelids to allow the eyelids to close.
The nerves and blood vessels are attached and the gracilis and latissimus dorsi muscles are transplanted and sutured to the healthy facial nerve, hypoglossal nerve, trigeminal nerve, etc.
Function can only be restored once new nerves grow from the area where the nerve was sutured to the target tissue, so it may take more than a year to recover from surgery.
Furthermore, the facial nerve is a bundle of nerves that control the numerous muscles that create complex facial expressions, so it is impossible to connect them precisely one by one. Therefore, even if movement is successfully restored after surgery, it is often the case that the intended facial expression is not produced. Once movement has recovered, it is important to practice making facial expressions while looking in a mirror (rehabilitation).