Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
The Department of Cardiovascular Surgery at Medical Research Institute Kitano Hospital was established in 2007 and is currently staffed by experienced staff, all of whom are certified cardiovascular surgeons and board-certified specialist training instructors, including the third-generation Chief Director, Dr. Hideo Kanemitsu. As part of the Heart Center, we provide comprehensive cardiovascular surgery care, including emergency cases, 24 hours a day, in close collaboration with the Department of Cardiology. Each of our staff has 20, 30, or 40 years of experience in cardiovascular surgery at various facilities both in Japan and overseas. Working together as a team, we provide meticulous, safe surgical care for each patient. At the same time, we prioritize innovation and minimal invasiveness, striving to provide highly specialized surgical care, leveraging the nation's highest-level hybrid operating room (Photo 1) and dedicated cardiovascular surgery operating room (Photo 2), both of which were newly established within the hospital in September. Furthermore, our hospital is a general hospital with a tradition of nearly 100 years and a proven track record of providing high-level medical care across all departments. As a community-based "multidisciplinary treatment" center comprised of many excellent medical departments, we strive to provide safe, reliable surgical treatment that is easy to understand, with the support of Kyoto University.

When the coronary arteries, which supply oxygen and nutrients to the heart muscle, become narrowed or blocked, blood flow becomes insufficient, leading to angina pectoris (ischemic state) or myocardial infarction (necrotic state). The primary symptom is chest pain during exertion or at rest. While angina pectoris symptoms improve with rest and medication, myocardial infarction results in persistent chest pain due to blocked blood vessels, and the heart muscle becomes damaged (necrotic) and stops functioning. In the worst case, it can lead to death. The cause is arteriosclerosis, which is likely to progress in conditions such as high blood pressure, high cholesterol, and other lipid metabolism disorders, diabetes, obesity, and smoking. Treatment options include drug therapy (such as coronary dilators and antiplatelet agents), catheter intervention (PCI), and coronary artery bypass graft surgery (CABG). At our hospital, cardiologists and cardiovascular surgeons discuss and decide on treatment plans at a morning conference in the cardiac center. CABG increases blood flow by connecting the internal thoracic artery or vein graft (great saphenous vein of the leg) to the narrowed coronary artery (Figures 1 and 2). Traditionally, surgery was performed by stopping the heart using a cardiopulmonary bypass machine, but at our hospital, we perform "off-pump coronary artery bypass grafting," which uses a device called a stabilizer to suppress the movement of the coronary artery while the heart is beating, and anastomoses the graft (Figure 1). Whether to use a cardiopulmonary bypass (on-pump, ONCAB) or not (off-pump, OPCAB) is determined by considering the advantages and disadvantages of each method, and the method that is most appropriate for each patient is selected.
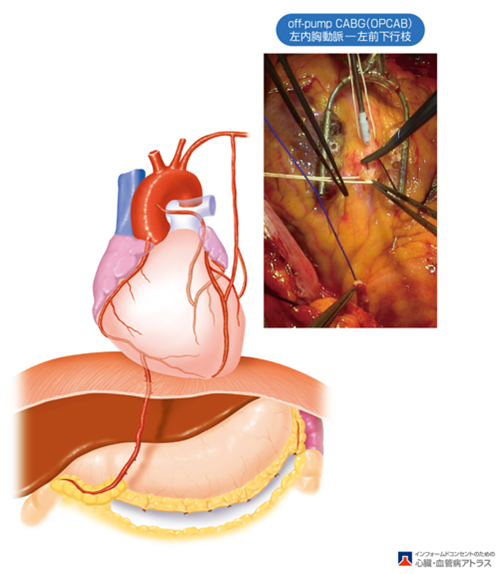
Figure 1. Left internal thoracic artery-left anterior descending coronary artery bypass (OPCAB) using a stabilizer and its schematic (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
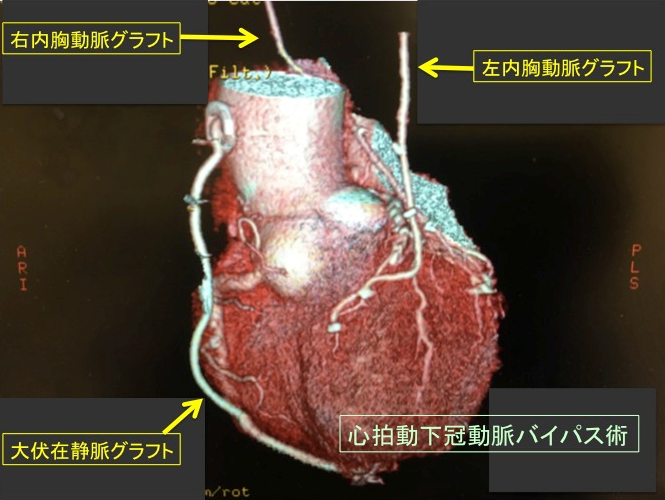
Figure 2. Contrast-enhanced CT image after coronary artery bypass surgery
The heart has four valves (Figure 3). Valve abnormalities include "stenosis," in which the valve stiffens and narrows, and "regurgitation (regurgitation)," in which the valve does not close properly, resulting in blood backflow (Figure 4). Both conditions begin with shortness of breath when climbing slopes or stairs, and as they worsen, they can develop into severe heart failure, including dyspnea at rest and generalized edema. Regurgitation, in particular, can lead to the development of "infective endocarditis," a systemic infection, and treatment is often difficult due to embolism or the sudden worsening of severe heart failure. Medical treatment for both stenosis and regurgitation is limited, and surgical treatment is recommended, especially for severe cases. Stenosis is treated with artificial valve replacement (prosthetic valve replacement) (Figure 5). Aortic stenosis has been increasing in recent years, particularly among elderly patients, and we are currently preparing to perform transcatheter aortic valve implantation and replacement (TAVI/TVAR) in our newly built hybrid operating room (Figure 6). On the other hand, for regurgitation (regurgitation), the first choice is valvuloplasty, which preserves and repairs the patient's own valves, such as the mitral, tricuspid, and aortic valves (Figure 7). Because valvuloplasty uses the patient's own valve, it offers superior valve function and long-term durability compared to prosthetic valves, and does not require anticoagulants (warfarin). While this procedure offers many benefits for patients, it also requires advanced techniques. While aortic valvuloplasty in particular requires specialized expertise, our hospital is actively promoting the new field of valvuloplasty, including aortic valvuloplasty and native valve-sparing root replacement (Figure 8). Additionally, there is minimally invasive treatment called mini-incision cardiac surgery (MICS) (Figure 7), and we are preparing to implement this procedure in the near future as a new development in our newly established dedicated cardiovascular surgery operating room.
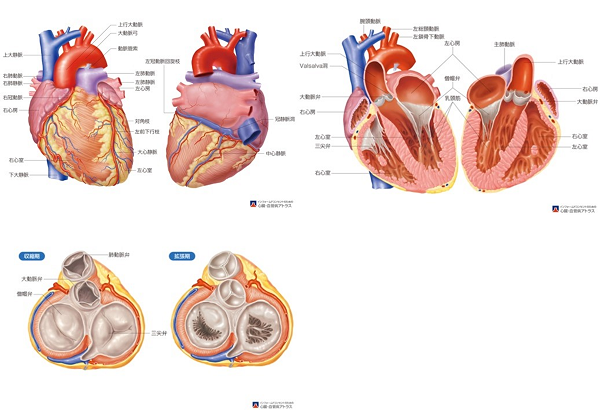
Figure 3. Internal structure of the heart (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
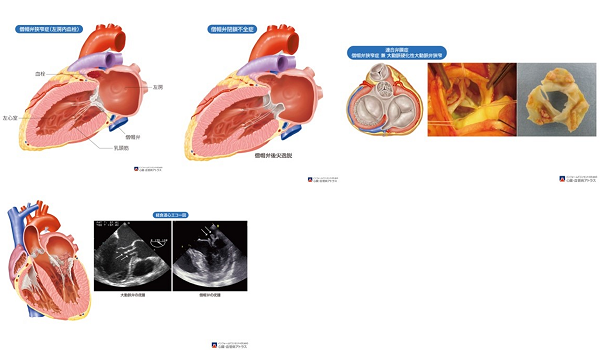
Figure 4. Valvular heart disease (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
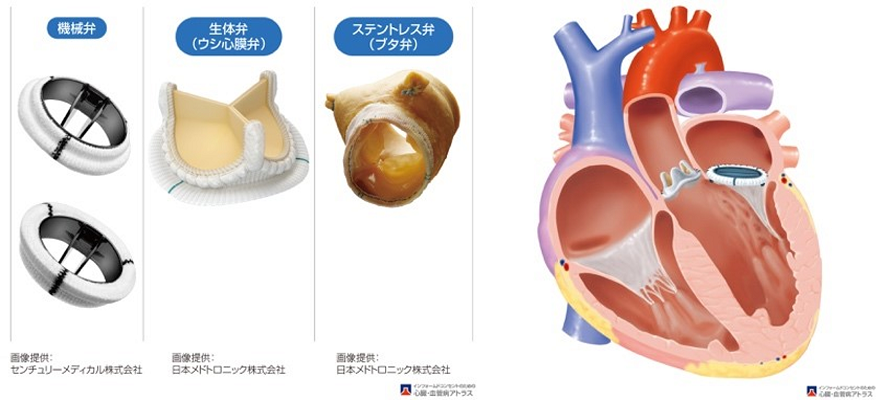
Figure 5. Artificial valves (left: mechanical valve, right: biological valve) and artificial valve replacement (aortic valve: biological valve, mitral valve: mechanical valve) (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
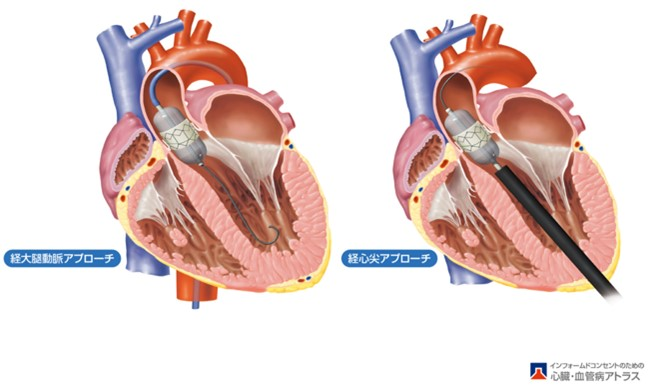
Figure 6 Transcatheter aortic valve implantation and replacement (TAVI/TAVR) (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
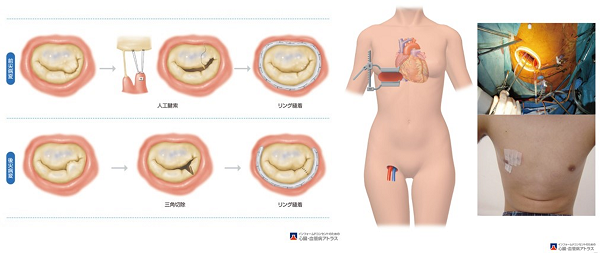
Figure 7 Mitral valve repair (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
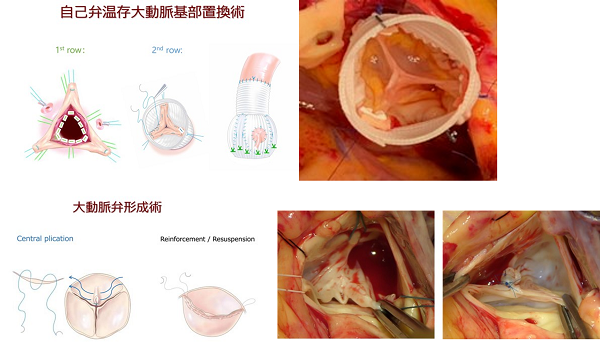
Figure 8. Aortic valvuloplasty and valve-sparing aortic root replacement (intraoperative photograph is a case from my previous workplace)
Aortic diseases include aortic aneurysms, aortic dissections, aortic injuries, and aortic stenosis/occlusion, with the first two being the most common. An aortic aneurysm is defined as an aortic diameter greater than 1.5 times the normal diameter (3 cm for the thoracic aorta and 2.5 cm for the abdominal aorta). Depending on the location, it is called a thoracic aortic aneurysm or abdominal aortic aneurysm. Thoracic aortic aneurysms (Figure 9) are further classified by location as ascending, arch, descending, and thoracoabdominal aortic aneurysms. Many aneurysms are asymptomatic until rupture (known as silent killers) and are often discovered incidentally during medical examinations or other medical tests. Atherosclerosis (degeneration) is the primary cause of aneurysms. The appropriateness of surgery is determined by factors such as aneurysm size (thoracic ≥ 5.5-6 cm, abdominal ≥ 5-5.5 cm), rate of expansion (expanding ≥ 5 mm over six months), and shape (saccular aneurysms, which are more likely to rupture, require earlier surgery than fusiform aneurysms). Medical treatment is limited to antihypertensive therapy to prevent enlargement and rupture, and no "miracle cure" has yet been developed. Surgical treatment is the only definitive cure, consisting of artificial vascular replacement (Figure 9) or minimally invasive transcatheter endovascular stent grafting (thoracic: TEVAR, abdominal: EVAR). On the other hand, aortic dissection is a condition that begins with sudden chest and back pain and causes a longitudinal tear at the medial level due to blood flow into the aortic wall through a tear in the intima (entry) (Figure 10). Because it can occur unexpectedly and without warning, even in aortas of normal diameter, and is associated with a high acute mortality rate (a silent killer), more appropriate initial treatment is required for lifesaving purposes. For Type A, emergency artificial vascular replacement is the first choice, while for Type B, conservative treatment or thoracic endovascular stent grafting (TEVAR) is the first choice, and prompt and appropriate treatment is desirable (Figure 11).
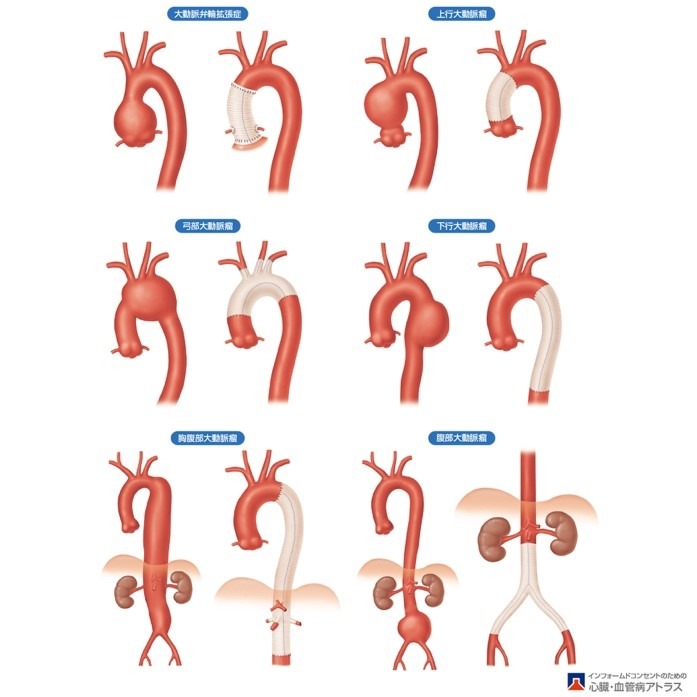
Figure 9 Thoracic and abdominal aortic aneurysms and artificial vascular replacement (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
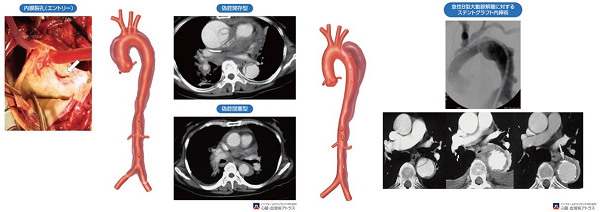
Figure 10 Aortic dissection: Type A and Type B (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
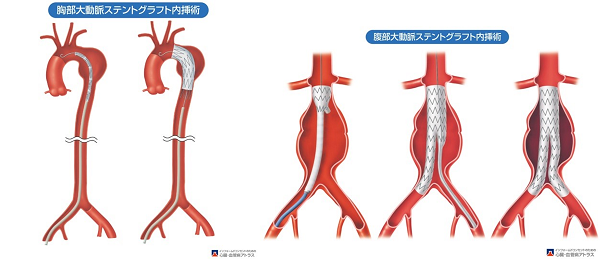
Figure 11. Thoracic and abdominal endovascular stent graft repair (TEVAR and EVAR) (Source: Yamashina, Chikamori,Ogino(Editor: Atlas of Cardiovascular Disease for Informed Consent)
Minimally invasive treatments for aortic aneurysms and dissections include (1) surgical procedures (artificial vascular replacement), as well as (2) transcatheter endovascular treatment using a metal stent-equipped endovascular (foldable) artificial blood vessel (called a stent graft) (Figure 11). These procedures are called EndoVascular Aortic Repair (EVAR) for the abdominal aorta and Thoracic EVAR (TEVAR) for the thoracic aorta. Nationwide, the proportion of artificial vascular replacements and TEVAR/EVAR is increasing, accounting for 40% of thoracic and 60% of abdominal procedures. Due to its minimally invasive nature (less physical strain), it is particularly suitable for high-risk cases and elderly patients. However, when TEVAR/EVAR is difficult due to anatomical conditions, we offer a hybrid treatment (3) in which bypass surgery (debranching) is performed first, followed by TEVAR and EVAR (Figure 12). At our hospital, we combine methods (1), (2), and (3) depending on the patient's condition. Furthermore, by performing the procedure in the latest hybrid operating room newly opened in September, it is possible to perform the procedure more accurately and safely (Photo 3). A similar minimally invasive treatment is transcatheter aortic valve implantation (TAVI/TAVR), which we are currently preparing to implement in collaboration with the Department of Cardiology.

Photo 3: Hybrid operating room
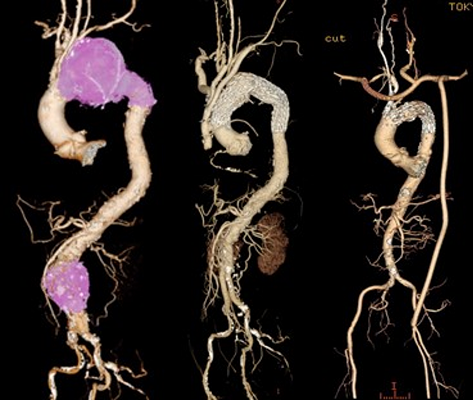
Figure 12 Hybrid aortic treatment (surgery + endovascular stent grafting): Experience at previous post
We are one of the few facilities that can provide surgical treatment for acute pulmonary thromboembolism, chronic pulmonary thromboembolism (CTEPH), and pulmonary artery sarcoma.

Figure 13. Excised specimen
We mainly perform Maze surgery for atrial fibrillation. At the same time, we prevent the occurrence of cerebral infarction by closure of the left atrial appendage clip. We also provide arrhythmia treatment in collaboration with the Cardiac Center's Arrhythmia Department.
We can also handle adult congenital heart disease, focusing on simple anomalies (malformations).
Visceral arterial disease also includes aneurysms and arterial dissections. While less common than aortic aneurysms and dissections, they carry the risk of rupture and require specialized treatment (aneurysmectomy, revascularization, or endovascular therapy). Peripheral vascular disease also includes diseases of the arteries and veins of the limbs. The former primarily involves arteriosclerosis obliterans (ASO), a condition characterized by stenosis or blockage due to arteriosclerosis, which reduces blood flow, causing leg muscle pain when walking (intermittent claudication), and ultimately requiring amputation of the lower limb due to necrosis (now called atherosclerotic LEAD). Depending on the patient's condition, we perform bypass surgery using vein grafts or artificial blood vessels, or catheter-based intervention (PTA), which uses balloons or stents to dilate narrowed or blocked arteries, in collaboration with the Cardiology Department at the Heart Center. Varicose veins, a common venous disease, are also treated surgically.
