Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
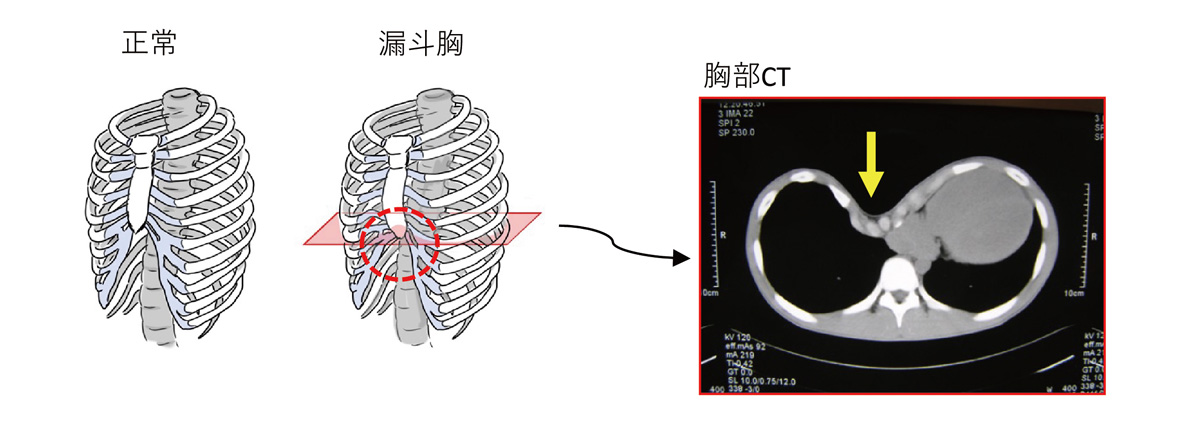
Pectus excavatum is a condition in which the center of the chest is sunken. It is believed to be caused by a deformed costal cartilage, but much remains unknown about the condition. While some people notice it from infancy, others notice it more as they grow, it is not a rare condition, occurring in approximately 1 in 1,000 people. It also runs in families and is thought to have a genetic component. Depending on the severity of the sunken chest, cold symptoms may persist or asthma-like symptoms may appear, but in many cases, the sunken chest is the only symptom observed in early childhood. After adolescence, chest pain and shortness of breath on exertion may be present. Even without physical symptoms, the sunken chest itself can pose significant psychological and social challenges, especially during school-age and adolescent years.

Exercises that open the chest, such as swimming, can increase lung capacity and improve the shape of the chest. While they are somewhat effective, they do not significantly improve the shape of the chest.
Patients with pectus excavatum often slouch because they are concerned about the depression in their chest, which makes the depression more noticeable. If the depression is mild, simply improving your posture can make it less noticeable.
This method involves attaching large suction cups to the anterior chest wall to apply negative pressure and lift the chest wall. It has been reported to be effective, but it needs to be continued daily for a long period of time (3 years).
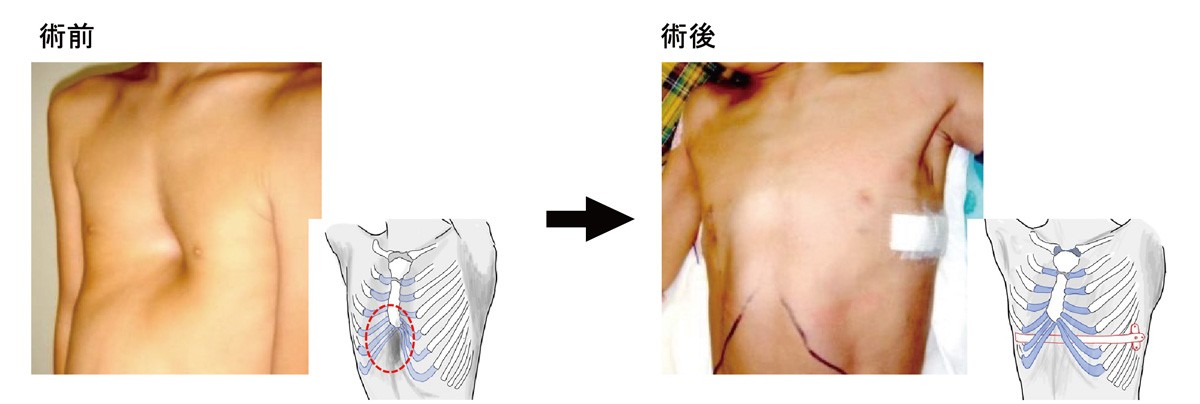
Our hospital performs the thoracoscopically assisted sternal lift (Nuss procedure), a minimally invasive surgical technique first reported by Dr. Nuss of the United States in 1998. A 3-4 cm skin incision is made on both sides of the chest, and a titanium bar is inserted behind the sternum to lift the depression from the inside. The hospital stay is approximately one week, but in adults, this may be extended for pain management reasons. The bar is surgically removed after one and a half to three years.
The scratches are on both sides so they are not very noticeable from the front.
The surgery is performed under general anesthesia. Since this surgery involves correcting bones, there is a lot of pain after the surgery. To suppress this pain, epidural anesthesia (anesthesia in which a thin tube is inserted between the spine and painkillers is continuously administered) is also used.
After surgery, rest is required to prevent the bar from slipping. Light exercise (radio calisthenics is a good guideline) can be resumed one month after surgery, and after three months, the bar will have stabilized and exercise restrictions will generally be lifted.
Many believe that surgery should be performed on children aged 12 or older, but in our experience, it is easier to correct the rib depression in younger children and there is less postoperative pain. After this surgery, rib deformity may become noticeable as the depression rises, but if surgery is performed during the growth period, the rib deformity can be expected to improve as the child grows after correction. While there is a high rate of recurrence of the depression if surgery is performed at this age, we address this issue by slightly overcorrecting the rib. Since exercise is restricted for approximately three months after surgery, the impact on school and work life must be considered. Surgery is possible even in junior high school and older, so we consult with the patient and their family to determine the appropriate timing for surgery.