Medical Research Institute KITANO HOSPITAL, PIIF Tazuke-Kofukai
Inquiry
search
close

Departments
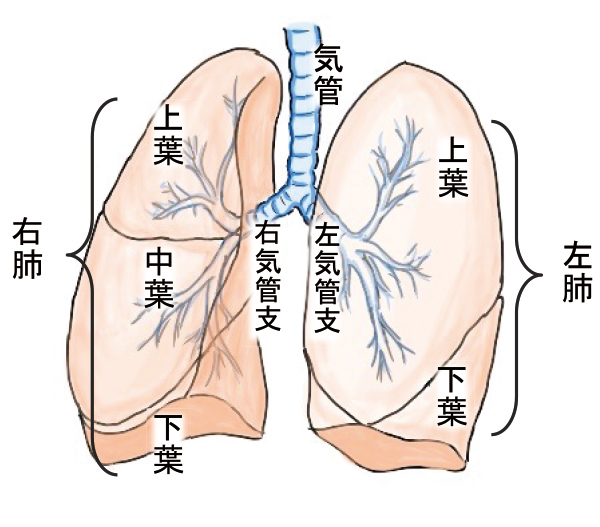
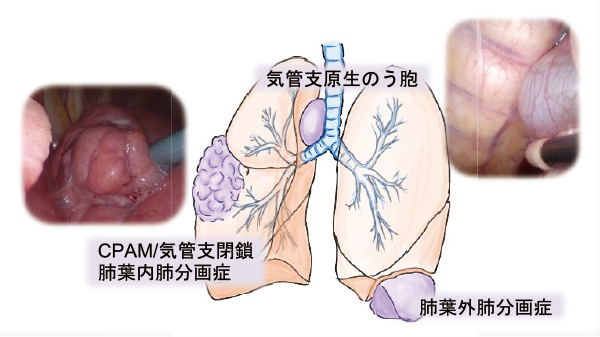
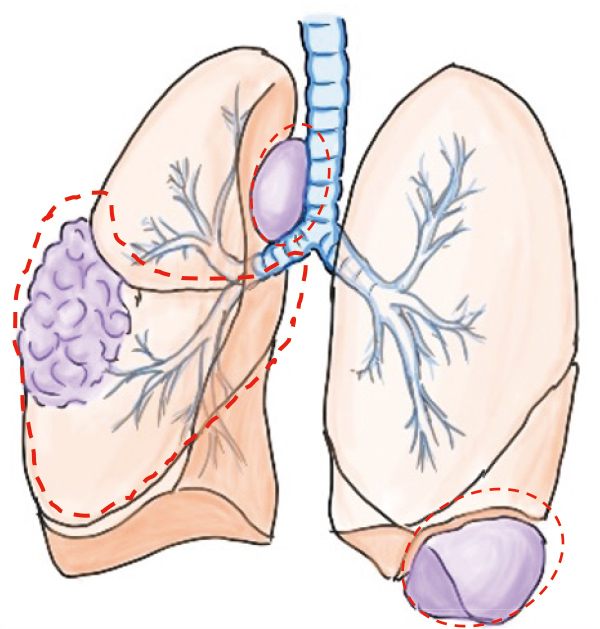
The organs involved in breathing include the trachea, bronchi, and lungs. The trachea leads to the left and right bronchi, each of which connect to the lungs. The right lung is divided into three lobes: the upper, middle, and lower lobes, while the left lung is divided into two lobes: the upper and lower lobes. During the process of forming the trachea, bronchi, and lungs, abnormal sac-like lesions (called cysts) can form. This is collectively called "congenital cystic lung disease." This includes bronchogenic cysts, congenital pulmonary airway malformations (CPAM), bronchial atresia, and pulmonary sequestration.
Bronchogenic cysts form adjacent to the trachea, while congenital pulmonary airway malformations (CPAM) and bronchial atresia occur inside the lungs. Pulmonary sequestration can be classified into two types: intralobar pulmonary sequestration, which occurs within the lung, and extralobar pulmonary sequestration, which occurs independently of the normal lung.
Respiratory organs
Congenital cystic lung disease
It is diagnosed through chest X-rays or CT scans taken when cold symptoms persist or when pneumonia develops. Some children remain asymptomatic, and may be diagnosed by chance when an X-ray is taken for another reason.
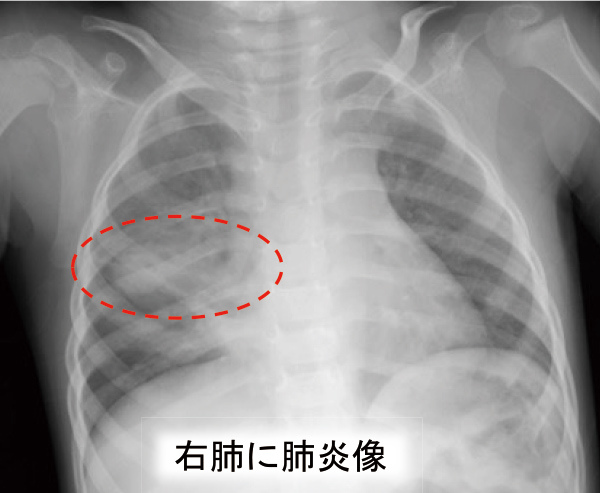

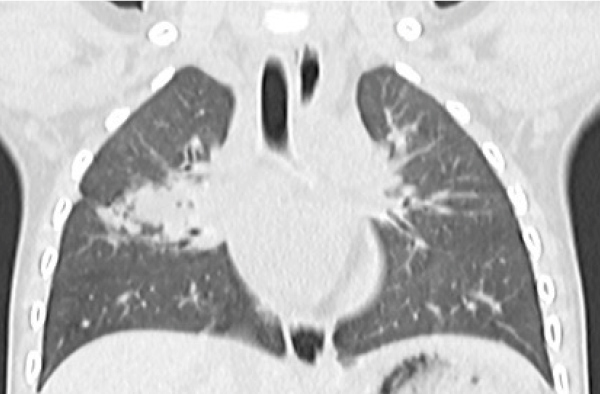
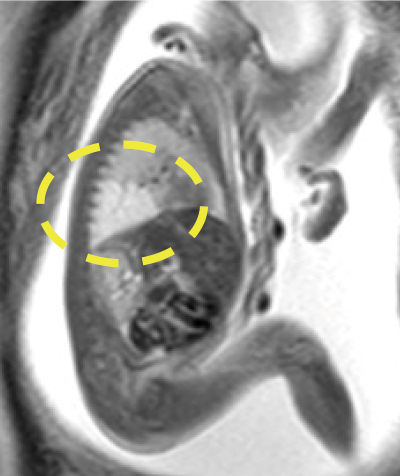
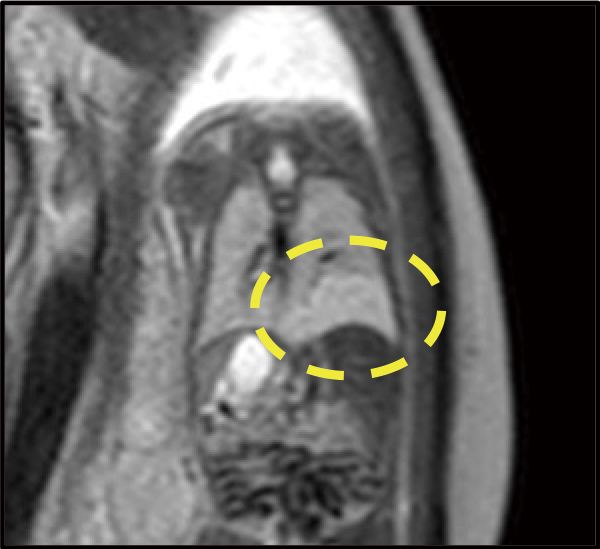
Congenital pulmonary airway anomalies (CPAM) were found hidden in the appearance of pneumonia.
In recent years, the quality of prenatal diagnosis has improved, and there are an increasing number of cases where lung abnormalities are detected before birth using fetal ultrasound. In the case of large cysts, there is a possibility that the cysts will compress the lungs after birth, causing respiratory problems, so it is necessary to prepare a sufficient system, including emergency surgery, before attempting delivery.

Surgery is required if symptoms are present. In cases of bronchogenic cysts and extralobar pulmonary sequestration, only the lesion is removed, but in cases of intrapulmonary lesions such as congenital pulmonary airway malformations (CPAM), it is difficult to remove only the lesion, and pediatric surgery generally involves performing a lobectomy, which involves the lung adjacent to the lesion as well. While some believe that asymptomatic children should be monitored without surgery, repeated bouts of pneumonia can cause adhesions within the chest, making surgery difficult. Ideally, removal should be performed before a pulmonary infection occurs, and our department recommends surgery around the age of one. Performing surgery during infancy allows the remaining lung to grow after surgery, allowing the child to acquire sufficient pulmonary function.
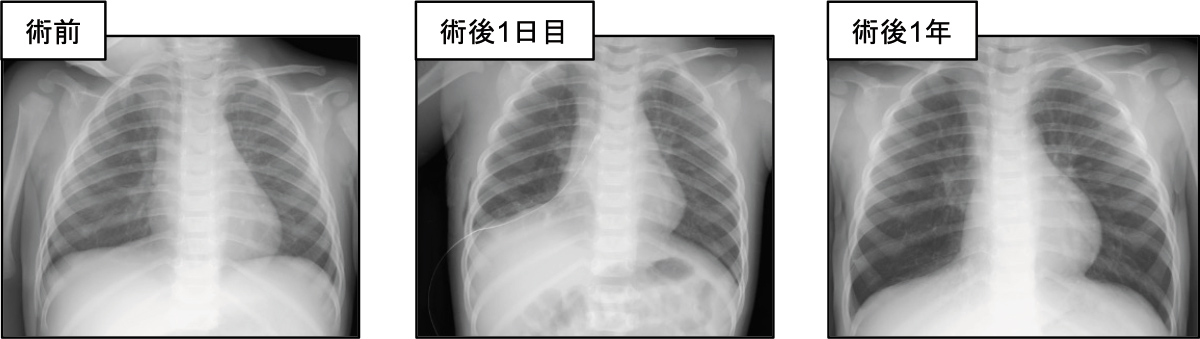
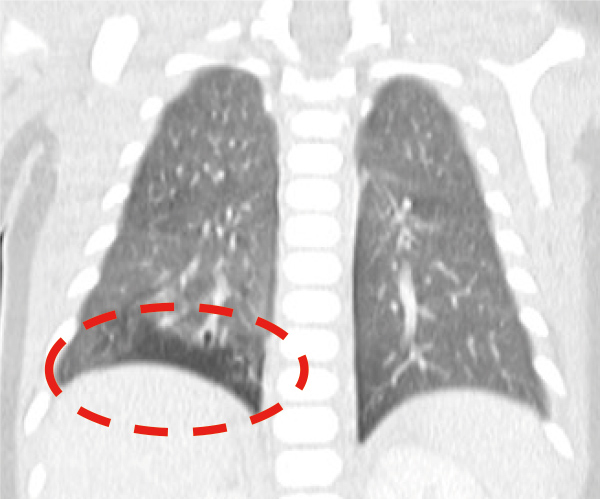
After right lower lobectomy. The right lung was smaller immediately after surgery, but one year later, the difference between the left and right lungs had disappeared.
In our department, we basically perform surgery using a thoracoscope. Because the incision is small, it puts less strain on the body and has cosmetic benefits. Also, open chest surgery requires a large incision in the muscles between the ribs, which is said to pose a risk of future spinal and thoracic deformation, and this is another good point as it can reduce this possibility.